| PANDEMIC ALERT LEVEL |
| 123456 |
| Tracking the next pandemic: Avian Flu Talk |
Ebola virus could reach USA by end of month |
Post Reply 
|
| Author | |
waterboy 
Valued Member 
Joined: January 21 2008 Status: Offline Points: 8170 |
 Post Options Post Options
") Thanks(0) Thanks(0)
 Quote Reply Quote Reply
 Topic: Ebola virus could reach USA by end of month Topic: Ebola virus could reach USA by end of monthPosted: September 04 2014 at 6:11pm |
|
Ebola Could Reach the U.S. By the End of This Month There is an 18 percent chance that a case of the Ebola virus will reach the United States by the end of September, according to a study published on Tuesday in PLOS Currents: Outbreaks. Despite restrictions reducing travel in and out of the infected countries by 80 percent, the study, which analyzes global flight patterns, suggests that a case of Ebola in the U.S. is becoming increasingly harder to avoid. It also lists the chance of the virus reaching the United Kingdom between 25 and 28 percent. The analysis also warns that if the current West African outbreak is not contained the likelihood of the virus reaching Europe and the U.S. will "increase consistently." The study lists just a five percent chance of Ebola occurring in the U.S. today, suggesting that the disease is far from contained to countries in West Africa. According to numbers obtained by the World Health Organization, there have been an estimated 3,685 cases and 1,841 deaths from the virus since the outbreak began. Although two Americans — Dr. Kent Brantley and Nancy Writebol — have been treated for Ebola in the U.S., both of them contracted the disease while working in Liberia. Doctors suggested that better medical care contributed to their eventual recovery. RELATED: No-Fun Dictator May Fine Boy for Ice Bucket Challenging Him A third infected American working in Liberia, Dr. Richard A. Sacra, is on his way to the U.S. for treatment. This article was originally published at http://www.thewire.com/global/2014/09/ebola-could-reach-the-us-by-the-end-of-this-month/379657/ |
|
 |
|
|
yogi1
V.I.P. Member 

Joined: August 12 2014 Location: Louisville, KY Status: Offline Points: 125 |
Post Options
Thanks(0)
Quote Reply
Posted: September 04 2014 at 8:46pm |
|
thanks for the heads up Waterboy. Good information.
I view this website cause I care for my family.
|
|
|
Duane W. Voss
|
|
|
|
|
Jen147
Moderator

Joined: March 23 2013 Status: Offline Points: 17144 |
Post Options
Thanks(0)
Quote Reply
Posted: September 05 2014 at 5:31am |
|
Me too yogi1... & because you can't get this comprehensive of a view of the "big picture" anywhere else on the www.
|
|
|
|
|
Albert
Admin
Joined: April 24 2006 Status: Offline Points: 47746 |
Post Options
Thanks(0)
Quote Reply
Posted: September 05 2014 at 5:55am |
|
If the crud hits the fan - no need to worry and we will work together in every area. We all have a significant advantage over the rest of the world in this area as this is our area of expertise.
|
|
|
https://www.facebook.com/Avianflutalk
|
|
|
|
|
Rome_is_burning
Guest Group 
|
Post Options
Thanks(0)
Quote Reply
Posted: September 05 2014 at 6:00am |
|
I think this is the original article with the stats and a map
http://currents.plos.org/outbreaks/article/assessing-the-international-spreading-risk-associated-with-the-2014-west-african-ebola-outbreak/ - http://currents.plos.org/outbreaks/article/assessing-the-international-spreading-risk-associated-with-the-2014-west-african-ebola-outbreak/ |
|
|
|
|
Albert
Admin
Joined: April 24 2006 Status: Offline Points: 47746 |
Post Options
Thanks(0)
Quote Reply
Posted: September 05 2014 at 6:13am |
|
Welcome to the forum Rome_is_Burning, lol. Like the handle there. Anyway - great find and thanks for posting the link. It's a long read, but here's a portion.
Background: The 2014 West African Ebola Outbreak is so far the largest and deadliest recorded in history. The affected countries, Sierra Leone, Guinea, Liberia, and Nigeria, have been struggling to contain and to mitigate the outbreak. The ongoing rise in confirmed and suspected cases, 2615 as of 20 August 2014, is considered to increase the risk of international dissemination, especially because the epidemic is now affecting cities with major commercial airports. Method: We use the Global Epidemic and Mobility Model to generate stochastic, individual based simulations of epidemic spread worldwide, yielding, among other measures, the incidence and seeding events at a daily resolution for 3,362 subpopulations in 220 countries. The mobility model integrates daily airline passenger traffic worldwide and the disease model includes the community, hospital, and burial transmission dynamic. We use a multimodel inference approach calibrated on data from 6 July to the date of 9 August 2014. The estimates obtained were used to generate a 3-month ensemble forecast that provides quantitative estimates of the local transmission of Ebola virus disease in West Africa and the probability of international spread if the containment measures are not successful at curtailing the outbreak. Results: We model the short-term growth rate of the disease in the affected West African countries and estimate the basic reproductive number to be in the range 1.5 − 2.0 (interval at the 1/10 relative likelihood). We simulated the international spreading of the outbreak and provide the estimate for the probability of Ebola virus disease case importation in countries across the world. Results indicate that the short-term (3 and 6 weeks) probability of international spread outside the African region is small, but not negligible. The extension of the outbreak is more likely occurring in African countries, increasing the risk of international dissemination on a longer time scale. Funding StatementWe acknowledge funding from DTRA-1-0910039 and MIDAS-National Institute of General Medical Sciences U01-GM070749. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.IntroductionThe outbreak of Ebola virus disease (EVD) that started in December 2013 has defied several months of mitigation and containment efforts. In July 2014 it was still evolving in Guinea, Liberia and Sierra Leone. As of 20 August, the toll in those countries had reached 844 EVD confirmed deaths 1. On 20 July, the outbreak reached Nigeria through an infected traveler coming from Liberia. The Nigerian official reports list 12 probable cases, and it is not clear if the outbreak has been contained. EVD is caused by infection with a virus of the family Filoviridae, genus Ebolavirus 2. EVD transmission during the incubation period is very unlikely and occurs via direct contact with blood, secretions, and/or other bodily fluids of dead or living infected persons. Gene sequencing of the virus causing the 2014 West African (2014WA) outbreak has demonstrated 98% homology with the Zaire Ebola virus, with a 55% case fatality ratio (CFR) across the affected countries 3. Unfortunately there are no licensed treatments available for EVD, and severely ill patients can only be cared for with intensive supportive care. The 2014WA outbreak is the largest ever observed, both by number of cases and geographical extension. For this reason, on 6-7 August, an Emergency Committee of the WHO 4 advised the 2014WA outbreak constitutes an ’extraordinary event’ and a public health risk to other States. Indeed, although the outbreak started in an isolated region of Guinea, transmission has occurred in large cities (Conakry, Freetown, Monrovia and Lagos) of the four affected countries. These urban areas have major international airports, thus raising concern about a quick internationalization of the outbreak (see Fig. 1). While importation of cases should not generate large outbreaks in countries where prompt isolation of cases in appropriate health care facilities occurs, it is clear that a quantitative analysis of the risk of importation of cases (likelihood, timeline, number of cases) in countries not affected at the moment by the outbreak may provide valuable intelligence on the evolution of the 2014WA outbreak. So far most of the analyses on the risk of international spread of the outbreak have focused on the analysis of the sheer volume of international passenger traffic across countries 5,6. These analyses however do not consider the local evolution of the outbreak in the affected countries and the specific etiology of the disease (incubation time scale, etc.). Here we provide a quantitative assessment of the international spread based on large-scale computer microsimulations of the 2014WA outbreak that generate stochastic simulations of epidemic spread worldwide, yielding, among other measures, the case importation events at a daily resolution for 3,362 subpopulations in 220 countries. We use the Global Epidemic and Mobility Model that integrates high-resolution data on human demography and mobility on a worldwide scale in a metapopulation stochastic epidemic model 7,8,9. The disease dynamics within each population consider explicitly that EVD transmissions occur in the general community, in hospital settings, and during funeral rites 10. For parameter inference, we use a Monte Carlo likelihood analysis that considers more than 1,000,000 simulations that sample the disease model space and the data on the 2014WA outbreak up to 9 August 2014. This approach selects the disease dynamic model that we use to generate numerical stochastic simulations of an epidemic’s local (within West African countries) and global progression. We evaluate the progression of the epidemic in West Africa and its international spread under the assumption that the EVD outbreak continues to evolve at the current pace. The numerical simulation results show a steep increase of cases in the West Africa region, unless the transmissibility of the EVD is successfully mitigated. The overall basic reproductive number of the epidemic in the region is estimated to be in the range 1.5 − 2.0. We find that, although surveillance and containment measures have been in place for several months, the transmissibility in hospital and funeral rites are likely an appreciable component of the overall transmissibility. The probability of case exportation is extremely modest (upper bound less than 5%) for non-African countries, with the exception of the United Kingdom (UK), Belgium, France and the United States (US). As of the beginning of September, the countries with the largest probability of seeing the arrival of EVD cases are Ghana, UK and Gambia. The overall probability of international spread will increase if the Nigerian outbreak is not promptly controlled. We also show that as of the end of September, the size distribution of outbreaks due to the international spread of the EVD is contained (median value <4 cases) for countries outside of the African region. Severe travel restrictions to and from the affected areas (80% airline traffic reduction) generates only a 3-4 weeks delay in the international spreading. The lack of detailed data on the 2014WA EVD outbreak makes any modeling approach vulnerable to the many assumptions and uncertainty about basic parameters and the quality of data. However, we hope that the characterization of the EVD 2014WA outbreak and the associated risk of international spread provided here may be useful to national and international agencies in allocating resources for interventions to contain and to mitigate the epidemic. 
Fig. 1: Air traffic connections from West African countries to the rest of the worldAir traffic connections from West African countries to the rest of the world. Guinea, Liberia, and Sierra Leone are not well connected outside the region. Nigeria, in contrast, being the most populous country in West Africa with more than 166 million people, is well connected to the rest of world. For historical reasons, all these countries have the strongest ties with European countries. ResultsTo provide a quantitative analysis of the risk of international spread of the EVD 2014WA outbreak, we use a data-driven global stochastic and spatial epidemic model 7,8,9. Details of the models are reported in the Methods section. The model generates microsimulations at the individual level that provide a stochastic ensemble of possible epidemic evolutions for each identical set of initial conditions and disease parameters. These simulations can be used to provide statistical estimates as newly generated cases, importation events, and time of arrival of the infection whose values depend on the key disease parameters determined by the calibration of the model. The adopted EVD modeling scheme 10 includes hospitalized and funeral compartments. To further support the obtained results we also considered a parsimonious susceptible, exposed, infectious and recovered (SEIR) disease scheme 11. We have considered the transmissibility component as the key parameter to be determined from data. We have also considered the current CFR (55%) from the 2014WA outbreak data 1. The remaining parameters (reported in the Methods section) follow from the study of Legrand et al. 10 and are consistent across the modeling literature for different outbreaks 11,12. 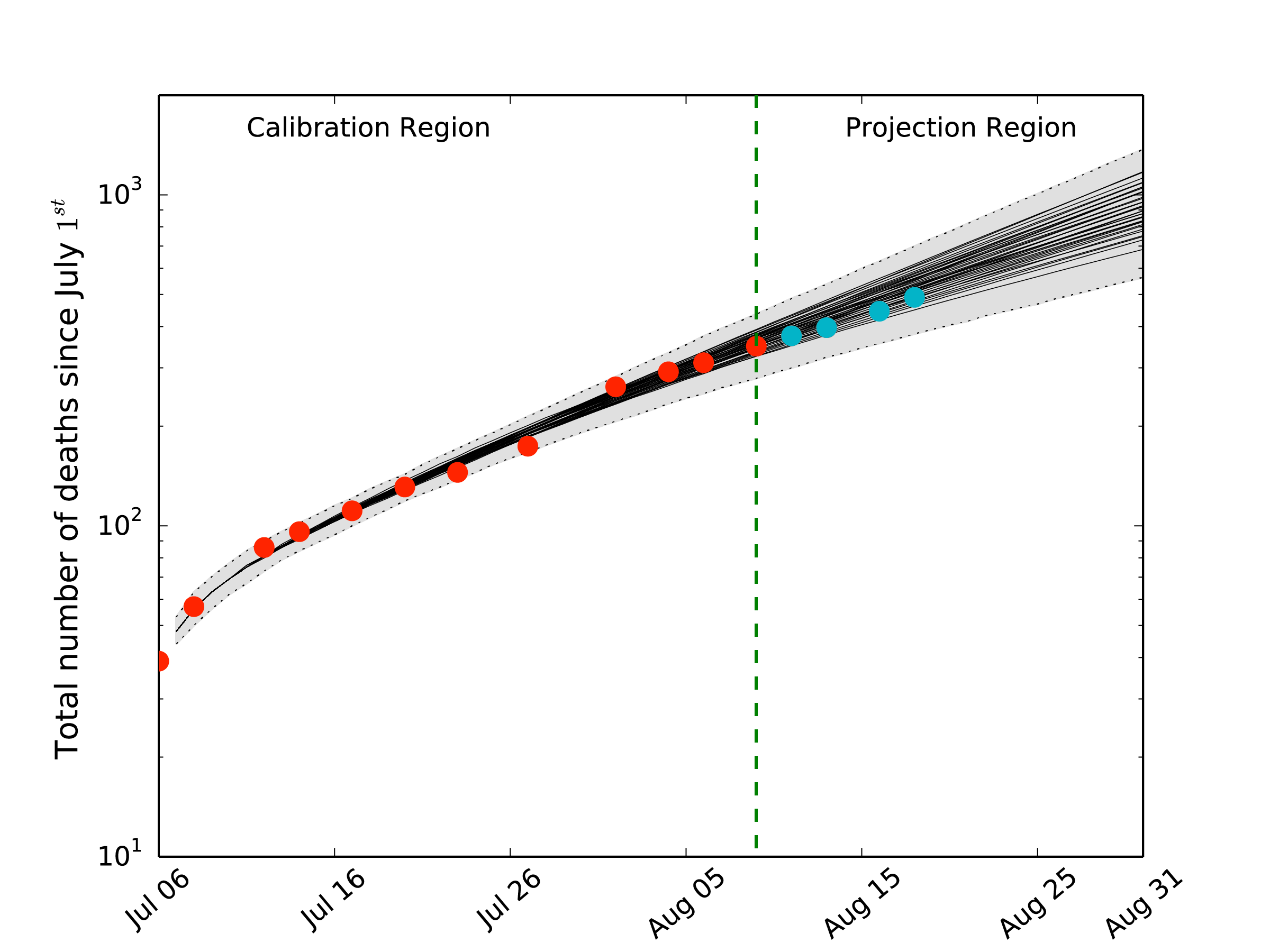
Fig. 2: Cumulative number of EVD deaths in West Africa as of 1 July 2014Cumulative number of EVD deaths in Sierra Leone, Guinea and Liberia as of 1 July 2014. The dots correspond to the data from the official WHO reports. The red dots were used for the model calibration. The blue dots are experimental data points received after the calibration of the model and are reported for the purpose of comparing with the model projections. The black thin lines are the expected values for the models selected by the likelihood analysis. The grey areas correspond to the 95% reference range provided by the fluctuations of the stochastic microsimulations. The green line divides the WHO data region used for the model selection from the projection region. 
Fig. 3: Risk of EVD case importationTop 16 countries at risk of EVD case importation in the short term: (top) 1 September and (bottom) 22 September 2014. The risk is assessed as the probability that a country will experience at least one case importation by the corresponding date, conditional on not having imported cases prior to 21 August 2014. The dark blue and light blue bars represent the minimum and maximum probability estimates, respectively, according to different models of case detection during travel (see text). The orange area corresponds to the probability maximum assuming the Nigerian outbreak starts to follow the same dynamic of the other West African countries affected by the EVD epidemic. We report the rank of Nigeria as well, which has experienced already a case importation on 20 of July and indeed it ranks among the countries with the larger probability of case importation. 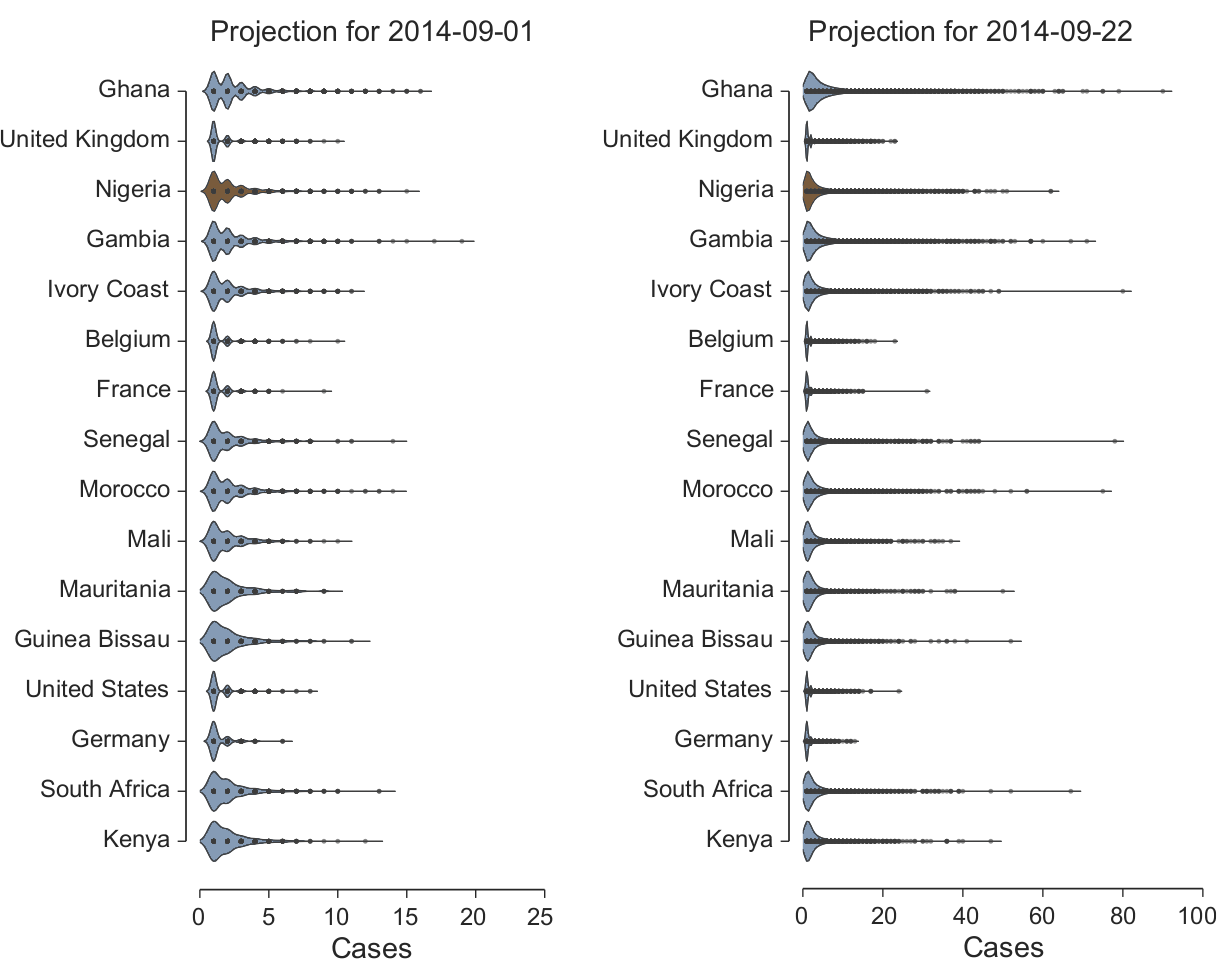
Fig. 4: EVD outbreak size distributionKernel density plots reproducing the distribution of the EVD outbreak size in countries that experience case importation at two different dates: (left) 1 September, (right) 22 September, conditional on not having imported cases prior to 21 August 2014. The outbreak size considers the imported case(s) and the local transmission events. The distribution is obtained by analyzing 10,000 microsimulations of the models selected by the relative likelihood analysis. The dots inside the violin plots represent distribution points. The same plots for the case in which the outbreak in Nigeria is not contained show small variations that do not alter the overall picture. Local transmission and the EVD dynamic in West Africa To estimate the key parameters, we consider data after 7 July 2014. As of that date, the outbreak had already been unfolding for several months and we can consider that interventions to reduce transmission were already in place, and thus included in the effective value of the transmissibility. By using the approach detailed in the Methods section for the EVD model including hospital and funeral settings 10, we estimate an overall basic reproductive number R0 = 1.8 [1.5 − 2.0] (interval at the 1/10 relative likelihood). The parsimonious SEIR model estimates R0 = 2.1 [1.9 − 2.4], although its relative likelihood is less than 1/100. In the Legrand et al. model 10 the basic reproductive number can be written as the sum of three terms relative to the transmission in the community, hospital and funeral settings, yielding RI = 0.8 [0.3 − 0.9], RH = 0.4 [0.2 − 1.4] and RF = 0.6 [0.2 − 1.0], respectively. The results suggest that although containment measures have been in place for several months, the likelihood of appreciable transmission in all settings is relevant. It must be noted however that the transmissibility in the various settings is difficult to determine as different partitions of the transmissibility can provide similar growth rates for the epidemic, and the available data may not be enough to discriminate otherwise. In Fig. 2 we plot the average behavior of the selected models compared to the WHO official data. The new data collected from the WHO after 9 August are within the 95% reference range of the projected behavior. Although this hints that the model is capturing the EVD dynamic in the West African regions, it also indicates that surveillance and containment measures are not yet sufficiently lowering the transmission rate to push the number of observed cases below the projected value. International spread The microsimulations generated by the selected models allow tracking the importation of EVD cases to other countries of the world from the West African countries affected by the outbreak. Concurrently to modeling the evolution of the EVD in the affected countries, our computational approach simulates the number of passengers traveling daily worldwide on each airline connection in the world. To quantify the risk of international spread, we consider the models selected with the multimodel selection approach to best represent the local EVD dynamic in West Africa and perform for each model 1,000 microsimulations. In each microsimulation, we monitor the arrival of EVD exposed individuals in countries across the world at a daily scale and estimate the probability of each country being invaded on 1 and 22 September 2014. These probabilities are conditional on the fact that no countries had confirmed EVD importation until 21 August 2014. We have also taken into account that Ivory Coast, Senegal, Guinea and Mauritania have closed their borders with the EVD affected area. Concerning Nigeria, we consider two scenarios: the first one in which the outbreak is contained, and one in which outbreak follows the same dynamic of EVD in Sierra Leone, Liberia, and Guinea. Furthermore, in assessing case importation by airline travel it is also important to consider if the EVD cases are detected during a connecting flight or at the final destination of the traveler. In our analysis we have implemented two different models: i) the EVD cases are identified after the first connecting flight; ii) the EVD cases are able to travel to their final destination. These models provide a minimum and maximum for the probability of case importation in each country, whose spread depends on whether the country’s transportation systems act as a traffic gateway or a destination hub. In Fig. 3 we report the top 15 countries plus Nigeria ranked according to their probability of case importation, conditional on the fact that they have not seen imported cases before August 21 (probability of case importation for countries not reported in the figure is available upon request to the authors). We also show the risk of importation for Nigeria. Although Nigeria has already received one case importation, it is relevant in supporting the obtained results to observe that it ranks as one of the countries with the largest probability of importation. It is possible to observe that the probability of importation is relatively small (<5%) for countries not in the African region, with the exception of the United Kingdom (UK). The probability of importation in a four weeks horizon (22 September) increases, but does not exceed the 25% threshold with the exception of Ghana and Gambia. It is important to stress that since we are talking of cumulative probabilities, they shall be constantly recalculated conditional on the fact that the importation has not been observed up to a given date. The risk of importation increases if the Nigerian outbreak is not contained. However the increase is more notable for the 22 September projection, as the Nigerian outbreak is very recent and needs time before it can add a critical mass of EVD cases to the spreading dynamics. In the results of Fig. 3 we do not take into account that some airlines have already decided to interrupt connections to the EVD-affected region. This analysis has to be considered as a baseline case where no traveling interventions are considered. For this reason we performed a sensitivity analysis in which we considered an 80% airline traffic reduction from and to the West African countries affected by the outbreak. The results obtained show a considerable reduction of the probability of case importation. However the probability of importation increases with time, and the net effect is essentially a mere three-week shift in the time progression for the probability of case importation (results not shown). A further quantity we can monitor is the number of imported and locally generated cases we can expect in each country conditional on the event of case importation. When an EVD carrier is arriving in a country not affected by the outbreak, we look at the local transmission and measure the size of the epidemic cluster generated by the index case. We assume that in countries outside Africa, the hospital and funeral transmissibility is null. This assumption, perhaps optimistic, is motivated by the current worldwide awareness of the possibility of EVD cases and the alert of public health agencies worldwide. Furthermore at this stage, we are interested in the risk of international spread from the West Africa region, and it is too early to make any inference about transmissibility of the disease in other socio-cultural settings. In Fig. 4 we show the kernel density plots of the distribution of the outbreak size, conditional on the occurrence of importation of EVD cases, for the top 16 countries at risk of importation (Fig. 3). We observe that the expected value of the cluster size in the case of international spread is always rather small (in all countries mean<6; median<4). Large outbreak involving more than 10 individuals although potentially possible can be considered as very rare events (Detailed statistics per country are available upon request). This numerical evidence is good news, as it points out that effective management and isolation of cases is keeping the number of EVD cases to deal with to a very limited number, lowering the risk of losing control of the outbreak. |
|
|
https://www.facebook.com/Avianflutalk
|
|
|
|
|
Rome_is_burning
Guest Group
|
Post Options
Thanks(0)
Quote Reply
Posted: September 05 2014 at 6:37am |
|
Thanks Albert I have been lurking here since the h1n1
outbreak in 09. I think this was my
first post though but I do feel as if I know most of you here from reading the forums
the last 5 years .
|
|
|
|
|
roni3470
Adviser Group

Joined: August 30 2006 Location: Colorado Status: Offline Points: 5390 |
Post Options
Thanks(0)
Quote Reply
Posted: September 05 2014 at 10:38am |
|
Is it just me??? I don't think 18% is that high!
|
|
|
NOW is the Season to Know
that Everything you Do is Sacred |
|
|
|
|
onefluover
Admin Group

Joined: April 21 2013 Location: Death Valleyish Status: Offline Points: 20151 |
Post Options
Thanks(0)
Quote Reply
Posted: September 05 2014 at 11:25am |
|
18% is greater odds than playing Russian Roulette with a 6-shooter. And that's 18% over a given timeframe that will be repeated over and over with that percentage also growing higher every day. It is with mathematical certainty many times over it will come here and everywhere else. The Pigmies might luck out.
|
|
|
"And then there were none."
|
|
|
|
|
Post Reply
|
|
 Tweet
Tweet
|
| Forum Jump | Forum Permissions You cannot post new topics in this forum You cannot reply to topics in this forum You cannot delete your posts in this forum You cannot edit your posts in this forum You cannot create polls in this forum You can vote in polls in this forum |








 Topic Options
Topic Options