| PANDEMIC ALERT LEVEL |
| 123456 |
| Tracking the next pandemic: Avian Flu Talk |
If you don't think its bad out there, read this. |
Post Reply 
|
| Author | ||
Tabitha111 
Adviser Group 

Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
 Post Options Post Options
") Thanks(1) Thanks(1)
 Quote Reply Quote Reply
 Topic: If you don't think its bad out there, read this. Topic: If you don't think its bad out there, read this.Posted: March 24 2020 at 4:36pm |
|
|
I am a hospitalist NP who was on call/admitting for 2 sister community hospitals in Los Angeles. This was MY 7p-7a shift last night (shift 7 out of 7). Sh*t is getting real: - Patient A on medsurg has cardiac arrest and got intubated; transferred to ICU; then emergent HD, bicarb, pressors, etc. - Patient B in DOU has RRT, transferred to ICU in full blown ARDS; intubated, pressors, multiple vent adjustments, etc. - Admit Patient C who arrived in respiratory failure and got intubated in the ER; pressors, acute MI, etc. - Call ICU charge RN as ICU beds are filling up and tell her to start looking into who we can downgrade. - Admit Patient D who also arrived in respiratory failure and got intubated in ER, but... ...ICU beds are all full, so we downgrade whoever we can STAT. This takes some time as we wait on labs and tests. - Elevator to RT office becomes inoperable, is shut down, and we run out of ventilators because we cannot move them without the elevator. - Meanwhile, a colleague texts me that she’s sending Patient E from SNF in respiratory failure to ER to be admitted and likely intubated. Great timing. Still no ICU beds or vents, so I call the SNF to try to divert ambo to our sister hospital, but ambo just left. SNF nursing tries to call ambo to redirect them as well. I call ER at sister hospital and give them heads up. - Engineering, RTs, and men with muscles are begged to carry 2 ventilators by hand down a stairwell to the ICU. 🙌🏼🙌🏼🙌🏼🙌🏼 (Despite spending half my night in the ICU, I round on the ICU at least 3 more times to check on everyone throughout the night. Also check in on every other unit as well). - Paged by ER for two telemetry admissions for chest pain and syncope. Phew ok that's easy. - While I’m putting in admission orders, Patient F who is chilling in ICU on BIPAP has PEA arrest out of nowhere. ER physician starts code, intubates patient (good thing I had the guys bring down an extra ventilator...just in case), he gets ROSC and loses it 3x. I take over code, multiple rounds, shock, drugs, etc. Same thing. While I am coding this Pt, ER at sister hospital pages me multiple times to admit Patient E who I diverted to them earlier in the night. - Finish code and H&P notes, check in once more on the ICU, and get ready to go home. - Patient A (s/p cardiac arrest) who I fixed up a lot through the night....arrests AGAIN and gets coded a second time. - Patient G who has been cruising comfortably on a ventilator in the ICU all week suddenly gets a massive spontaneous pneumo and needs a stat CT. - Finally, I make it home in time to catch the sunrise and a double rainbow, and work out with my personal trainer (in-home social distancing personal training of course!) NOT TODAY Coronavirus, NOT today. 💪🏽 |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
 |
||
|
KiminNM
V.I.P. Member
Joined: January 22 2020 Location: NM Status: Offline Points: 6605 |
Post Options
Thanks(0)
Quote Reply
Posted: March 24 2020 at 8:00pm |
|
|
I can't find the words to respond to this. Geezuz! was first, then "we're effed". Then just a huge sigh. Because it didn't have to be this way... |
||
|
||
|
Penham
Chief Moderator

Moderator Joined: February 09 2006 Location: United States Status: Offline Points: 14913 |
Post Options
Thanks(0)
Quote Reply
Posted: March 25 2020 at 9:22am |
|
|
Wow |
||
|
||
|
MamaBear4
V.I.P. Member

Joined: April 11 2007 Location: United States Status: Offline Points: 511 |
Post Options
Thanks(0)
Quote Reply
Posted: March 25 2020 at 10:37am |
|
|
🙏🏻 Hope and pray for the best prepare for the worst. In our area as probably most areas, when you go to the ER or go in 911 no one can go in with you so I thought its time for everyone to prepare for that. Everyone needs to write down or print medical history and medication list and pin it on their loved one before seeking medical care. Everyone will assume the hospital has their records but their systems may go down get hacked etc. Be prepared for every scenario. Don’t wait till you are unwell and not able to do it. Print it and have some safety pins ready. The medical professionals will see it and be very thankful when they change the patients clothes. This is extreme but even taking a sharpie and writing their name on their arm. They do that Pre surgery so no mistakes happen. Mistakes will happen. All we can do is our best.❤️ |
||
|
||
|
MamaBear4
V.I.P. Member
Joined: April 11 2007 Location: United States Status: Offline Points: 511 |
Post Options
Thanks(0)
Quote Reply
Posted: March 25 2020 at 10:47am |
|
|
Forgot to say Thank you Tabbitha111 for all you do and all Medial Professionals and 1st Responders. We are doing #SOLIDARITYAT8 every night. |
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 25 2020 at 12:37pm |
|
|
Just so you know, this is not me posting these stories, but they are from medical personnel on the frontlines. |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 25 2020 at 12:39pm |
|
|
From a nurse last night- |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
Sheep Lady
V.I.P. Member
Joined: February 06 2020 Status: Offline Points: 3215 |
Post Options
Thanks(0)
Quote Reply
Posted: March 25 2020 at 12:47pm |
|
|
The fact that you guys have the guts to keep showing up for work in this hell is incredible. Our govt has been so unprepared for so long and now it is catching up to them and all we hear is blame. Your precious lives are on the line and this is just so wrong. My prayers are for each and every one of you and your families. We respect you and love you for all you are doing. Beyond that, words fail me. |
||
|
Sheep Lady
|
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(1)
Quote Reply
Posted: March 26 2020 at 8:06pm |
|
|
FROM THE FRONTLINES: "I am an ER MD in New Orleans. Class of 98. Every one of my colleagues have now seen several hundred Covid 19 patients and this is what I think I know. Clinical course is predictable. 2-11 days after exposure (day 5 on average) flu like symptoms start. Common are fever, headache, dry cough, myalgias(back pain), nausea without vomiting, abdominal discomfort with some diarrhea, loss of smell, anorexia, fatigue. Day 5 of symptoms- increased SOB, and bilateral viral pneumonia from direct viral damage to lung parenchyma. Day 10- Cytokine storm leading to acute ARDS and multiorgan failure. You can literally watch it happen in a matter of hours. 81% mild symptoms, 14% severe symptoms requiring hospitalization, 5% critical. Patient presentation is varied. Patients are coming in hypoxic (even 75%) without dyspnea. I have seen Covid patients present with encephalopathy, renal failure from dehydration, DKA. I have seen the bilateral interstitial pneumonia on the xray of the asymptomatic shoulder dislocation or on the CT's of the (respiratory) asymptomatic polytrauma patient. Essentially if they are in my ER, they have it. Seen three positive flu swabs in 2 weeks and all three had Covid 19 as well. Somehow this ***** has told all other disease processes to get out of town. China reported 15% cardiac involvement. I have seen covid 19 patients present with myocarditis, pericarditis, new onset CHF and new onset atrial fibrillation. I still order a troponin, but no cardiologist will treat no matter what the number in a suspected Covid 19 patient. Even our non covid 19 STEMIs at all of our facilities are getting TPA in the ED and rescue PCI at 60 minutes only if TPA fails. Diagnostic CXR- bilateral interstitial pneumonia (anecdotally starts most often in the RLL so bilateral on CXR is not required). The hypoxia does not correlate with the CXR findings. Their lungs do not sound bad. Keep your stethoscope in your pocket and evaluate with your eyes and pulse ox. Labs- WBC low, Lymphocytes low, platelets lower then their normal, Procalcitonin normal in 95% CRP and Ferritin elevated most often. CPK, D-Dimer, LDH, Alk Phos/AST/ALT commonly elevated. Notice D-Dimer- I would be very careful about CT PE these patients for their hypoxia. The patients receiving IV contrast are going into renal failure and on the vent sooner. Basically, if you have a bilateral pneumonia with normal to low WBC, lymphopenia, normal procalcitonin, elevated CRP and ferritin- you have covid-19 and do not need a nasal swab to tell you that. A ratio of absolute neutrophil count to absolute lymphocyte count greater than 3.5 may be the highest predictor of poor outcome. the UK is automatically intubating these patients for expected outcomes regardless of their clinical presentation. An elevated Interleukin-6 (IL6) is an indicator of their cytokine storm. If this is elevated watch these patients closely with both eyes. Other factors that appear to be predictive of poor outcomes are thrombocytopenia and LFTs 5x upper limit of normal. Disposition I had never discharged multifocal pneumonia before. Now I personally do it 12-15 times a shift. 2 weeks ago we were admitting anyone who needed supplemental oxygen. Now we are discharging with oxygen if the patient is comfortable and oxygenating above 92% on nasal cannula. We have contracted with a company that sends a paramedic to their home twice daily to check on them and record a pulse ox. We know many of these patients will bounce back but if it saves a bed for a day we have accomplished something. Obviously we are fearful some won't make it back. We are a small community hospital. Our 22 bed ICU and now a 4 bed Endoscopy suite are all Covid 19. All of these patients are intubated except one. 75% of our floor beds have been cohorted into covid 19 wards and are full. We are averaging 4 rescue intubations a day on the floor. We now have 9 vented patients in our ER transferred down from the floor after intubation. Luckily we are part of a larger hospital group. Our main teaching hospital repurposed space to open 50 new Covid 19 ICU beds this past Sunday so these numbers are with significant decompression. Today those 50 beds are full. They are opening 30 more by Friday. But even with the "lockdown", our AI models are expecting a 200-400% increase in covid 19 patients by 4/4/2020. Treatment Supportive worldwide 86% of covid 19 patients that go on a vent die. Seattle reporting 70%. Our hospital has had 5 deaths and one patient who was extubated. Extubation happens on day 10 per the Chinese and day 11 per Seattle. Plaquenil which has weak ACE2 blockade doesn't appear to be a savior of any kind in our patient population. Theoretically, it may have some prophylactic properties but so far it is difficult to see the benefit to our hospitalized patients, but we are using it and the studies will tell. With Plaquenil's potential QT prolongation and liver toxic effects (both particularly problematic in covid 19 patients), I am not longer selectively prescribing this medication as I stated on a previous post. We are also using Azithromycin, but are intermittently running out of IV. Do not give these patient's standard sepsis fluid resuscitation. Be very judicious with the fluids as it hastens their respiratory decompensation. Outside the DKA and renal failure dehydration, leave them dry. Proning vented patients significantly helps oxygenation. Even self proning the ones on nasal cannula helps. Vent settings- Usual ARDS stuff, low volume, permissive hypercapnia, etc. Except for Peep of 5 will not do. Start at 14 and you may go up to 25 if needed. Do not use Bipap- it does not work well and is a significant exposure risk with high levels of aerosolized virus to you and your staff. Even after a cough or sneeze this virus can aerosolize up to 3 hours. The same goes for nebulizer treatments. Use MDI. you can give 8-10 puffs at one time of an albuterol MDI. Use only if wheezing which isn't often with covid 19. If you have to give a nebulizer must be in a negative pressure room; and if you can, instruct the patient on how to start it after you leave the room. Do not use steroids, it makes this worse. Push out to your urgent cares to stop their usual practice of steroid shots for their URI/bronchitis. We are currently out of Versed, Fentanyl, and intermittently Propofol. Get the dosing of Precedex and Nimbex back in your heads. One of my colleagues who is a 31 yo old female who graduated residency last may with no health problems and normal BMI is out with the symptoms and an SaO2 of 92%. She will be the first of many. I PPE best I have. I do wear a MaxAir PAPR the entire shift. I do not take it off to eat or drink during the shift. I undress in the garage and go straight to the shower. My wife and kids fled to her parents outside Hattiesburg. The stress and exposure at work coupled with the isolation at home is trying. But everyone is going through something right now. Everyone is scared; patients and employees. But we are the leaders of that emergency room. Be nice to your nurses and staff. Show by example how to tackle this crisis head on. Good luck to us all." |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
mccae73
Valued Member 
Joined: March 26 2020 Location: shit show Status: Offline Points: 40 |
Post Options
Thanks(0)
Quote Reply
Posted: March 26 2020 at 8:16pm |
|
|
i know this is totally out of the box but have you tried giving anybody speed |
||
|
||
|
mccae73
Valued Member
Joined: March 26 2020 Location: shit show Status: Offline Points: 40 |
Post Options
Thanks(0)
Quote Reply
Posted: March 26 2020 at 8:24pm |
|
|
A group of scientists from the National Health Research Institutes in Taiwan set out to study how methamphetamine interacts with influenza A virus in lung cells. Previous research has suggested that chronic meth abuse makes individuals more susceptible to pathogens such as HIV. The team wanted to investigate They took cultures of human lung epithelial cells, exposed them to different concentrations of meth and then infected them with an H1N1 strain of human influenza A. By 30 to 48 hours after infection, the meth-treated cells had a much lower concentration of the virus than the control group, the researchers reported. What's more, this reduction occurred in a dose-dependent manner, meaning the more meth, the less the virus reproduced. how the drug might reduce users' resistance to flu viruses. |
||
|
||
|
mccae73
Valued Member
Joined: March 26 2020 Location: shit show Status: Offline Points: 40 |
Post Options
Thanks(0)
Quote Reply
Posted: March 26 2020 at 8:26pm |
|
|
i know its super fucked up but its just an idea i mean dr s prescribe the same thing to kids |
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 26 2020 at 10:11pm |
|
|
From an ED Doc- COVID-19 HAS NOT BEEN CIRCULATING FOR MONTHS IN THE US I am seeing stories repeatedly posted suggesting this And I want to be clear, until about 2 weeks ago, I believed it to be true also In late December, January, and February, in ERs we saw a ton of patients come in who appeared to have a pretty bad case of the flu. They looked just like flu patients. But most of them tested negative for the flu. Many people recently have thought "Well maybe I had COVID-19" and some genetic studies have suggested that it's been here a little longer than we thought That is wrong. I don't really care what genetic studies say, because the answer is in the Emergency Rooms and ICUs I saw hundreds and hundreds of flu-like patients in Jan and Feb, and even though they were Flu negative, they were still pretty sick. But...NONE of them progressed to the type of critical illness we are seeing with COVID. And I mean none of them. I would work a shift in the ER and see 5-10 patients who all seemed like they had a bad flu, but were flu negative. But for the most part they were OK to go home, or if we brought them in they generally got better That is not what we are seeing with this. We are seeing patients who come in after 8-9 days of having a bad flu, suddenly getting much worse. With chest xrays and CT scan that look like a bomb went off in their lungs. With severe hypoxia. I can now look at a patient and look at a chest xray and predict with about 90% certainty whether that patient has COVID or not. And not one of them looks like the patients I saw in Jan/Feb I know everyone is looking for a little hope, but this is not where to find it. |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
WitchMisspelled
Adviser Group
Joined: January 20 2020 Status: Offline Points: 17170 |
Post Options
Thanks(0)
Quote Reply
Posted: March 27 2020 at 4:46am |
|
|
Good post, Tabitha. I count an ER and a critical care nurse among my circle of friends here in Brooklyn. They contradict what this doctor says. They both report there were patients in late December through January who tested flu negative and every bit as bad as we're seeing now. Perhaps a few dozen between late December through January. I don't know where this doctor is from, but nothing will convince me after talking with these two nurses that I made the wrong call that there was community spread here in NYC as early as February and began social distancing back then. |
||
|
||
|
Newbie1A
Adviser Group

Joined: January 26 2018 Location: Alberta Status: Offline Points: 11180 |
Post Options
Thanks(0)
Quote Reply
Posted: March 27 2020 at 10:48am |
|
|
I hope it's ok I post this here Tabitha, along same lines... |
||
|
If it's to be - it's up to me!
|
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 27 2020 at 1:13pm |
|
|
From the frontlines- Just wanted to share my current situation in primary care. I am a NP in primary care in Az. We have checked in on my pt many times since 3/18. She reported no improvement in her symptoms. I did not send her initially for a chest X-ray because I did not want to risk her exposing the virus to others at an imaging facility. Do to her worsening SOB I tried to get a stat chest X-ray and understandably the imaging facility would not take her. I chose to send her to the ER for evaluation and chest X-ray. And here we are 9 days waiting.... In primary care we are triaging our respiratory pts. Due to the fact we are unable to swab and do not have PPE we must operate safely by not seeing these types of pts. We have implemented telemed visits and are referring pts for swabs via mayo or banner if needed. Most pts are being advised to self quarantine, Tylenol, fluids, and rest. The above scenario regarding my assessment and care of this pt isn’t perfect and is hardly what I thought healthcare would ever look like in America. It is in my opinion a reason why AZ numbers are lower than one would expect and that contributes to why we do not have a shelter in place order here. I am praying for all of you, your pts, your family and friends ❤️ |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 28 2020 at 9:45am |
|
|
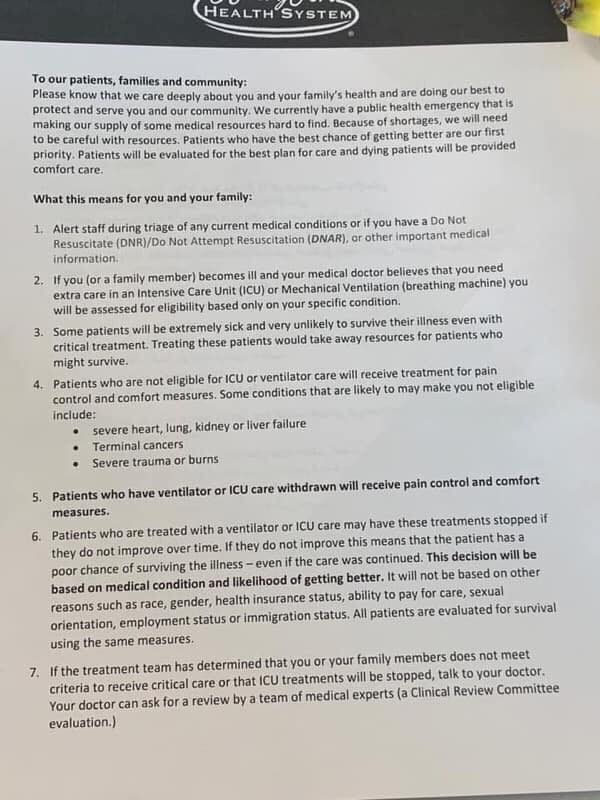
FROM THE FRONTLINES- |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 28 2020 at 12:12pm |
|
|
it's real, it's from Henry Ford Hospital...its from a draft that "escaped"
|
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
Penham
Chief Moderator
Moderator Joined: February 09 2006 Location: United States Status: Offline Points: 14913 |
Post Options
Thanks(1)
Quote Reply
Posted: March 28 2020 at 12:34pm |
|
|
You are not in a good position. I know our prisons are not allowing any visitation. There's no non- essential workers allowed to work right now, so any inmates on work release would not be working. So pretty much the only way they would get Covid-19 is from the guards bringing it in, same way most of the contraband comes in. |
||
|
||
|
Technophobe
Assistant Admin

Joined: January 16 2014 Location: Scotland Status: Offline Points: 88450 |
Post Options
Thanks(1)
Quote Reply
Posted: March 28 2020 at 12:37pm |
|
|
I've been expecting that from the start. Tragic - but not surprising. |
||
|
How do you tell if a politician is lying?
His lips or pen are moving. |
||
|
||
|
CRS, DrPH
Expert Level Adviser
Joined: January 20 2014 Location: Arizona Status: Offline Points: 26660 |
Post Options
Thanks(1)
Quote Reply
Posted: March 28 2020 at 12:40pm |
|
|
Thanks, my late father in law was a physician at Henry Ford Hospital, they have a sterling reputation. I think that nearly all US healthcare facilities will be following this type of guidance soon. We are basically in a war-time footing, so personnel and resources must be conserved. |
||
|
CRS, DrPH
|
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 28 2020 at 12:52pm |
|
|
just to be clear, it is not ME that are making these posts...i am gathering them from various health care workers across the nation to show a real picture of what is going on behind the scenes and behind the news reports... |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: March 28 2020 at 1:00pm |
|
|
A fairly long smattering of Health Care workers reports ON THE FRONTLINE: RR findings in general have little correlation with disease severity in pneumonia, and that goes for COVID as well. A patient <65 who isn't hypoxic or hypotensive with a RR <30 essentially never needs to be admitted for pneumonia outside of unique circumstances (regardless of imaging), and even then it's usually "just in case". I will say this disease does make one hesitate because of its unique course, but there are predictors other decompensation as you said that can guide you. I don't love the Plaquenil option and the data sucks to be honest, but I have used it some. Remdesivir really seems to work well in the severe cases from my anecdotal perch. Also, some of these patients have incredible IL-6 levels. I've never seen numbers this high even in my AIDS patients with KICS. One guy had a level above assay which were pretty sure has never been reported by our lab before. Obviously we dont know what they were for Spanish flu patients 100 years ago but the cytokine storm was the hallmark of that disease. We're seeing something similar here. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Patients requiring supplemental oxygen beyond regular nasal cannula, which in COVID usually ends up being a ventilator. We don't really try NIPPV as the OP said because it doesn't help much and risks aerosolizing the virus. I've had one patient saved from a vent by high flow nasal cannula, which in terms of pure oxygen delivery is the most we can provide prior to intubation, but generally these people are either on NC or getting intubated because the hypoxia becomes so profound so quickly if they crash. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ I've got several doc friends in NOLA that are giving identical stories. The kind of stuff you and they are talking about are things I'd never have expected to see as a physician. I went from seeing none of these patients, to 10 of them in the last 2 days. All of them so far mild. I'm sure that this will change in the next day or two. As i told some of my colleagues, based on the number of mild cases I'm seeing, **** is about to hit the fan. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ San Antonio. I think they state that we reportedly have only 67 confirmed cases currently, however, I can tell you that the large majority of patients that likely have it are being sent home without testing. I have seen 2 confirmed cases myself. Another 8 that either have a confirmed close contact with a +individual, labs and imaging results that are classic for the CV, or a very concerning travel history and symptoms that are consistent with it. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Hang in there. Unfortunately, I am hearing stories similar to this in areas around New Orleans. Let's hope things get better. Praying for you. This virus is just a bad monster. Once you go into cytokine storm it is so hard to survive. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ People asking about the hydroxycholoroquine combination, once you are this sick it is very unlikely to help. Way too much viral replication and inflammation has already occurred. It's purpose the way I see it is for us doctors in the community to get it started as soon as possible to hopefully slow down viral replication and inflammation so they never get to ventilator stage. Also hopefully it will be proven to successful in prophylaxis to protect the physicians l from getting too much viral exposure. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Based on what I'm hearing from colleagues in peds ID it seems like asthma is the theme of severe presentations under 20. Kids with asthma are the ones getting intubated, but thankfully this is more related to reactive airway disease and less so parenchymal lung disease. It basically causes a severe asthma exacerbation which is easy enough to fix once they're intubated. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Another day, another 5 seen, 2 are confirmed, the other 3 told they should assume they have it. Our hospital system is about to run out of rapid test kits and the local health department has asked us to no longer send them swabs from patients that are being discharged (that was apparently a thing for about 4 days before they were so inundated with swabs that they had to stop it). ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ All the cases so far have remained mild, thankfully, although I suspect most are early in the disease process. Ages range from 20-80+. Can't rely on the chief complaint to be the typical viral syndrome, as I have had one who came in for abdominal pain and another was an older gentleman with altered mental status. Many of them don't have fever. Several of them have pretty unremarkable lab work, although many have several of the typical lab or imaging abnormalities. Many of these patients are being seen by healthcare workers w/o proper PPE due to atypical complaints. One of the confirmed patients was brought in by EMS without any PPE on whatsoever, although I don't think they realized that this patient was at risk for having it. Unfortunately, after talking with some of my local EMS friends, they are getting absolutely no education regarding ways to protect themselves, and who they should suspect this in, at least according to them. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ On another note, I'm having to limit the quantity to dispense on certain inhalers and other maintenance medications for chronic conditions. We are having a lot of medications go on backorder and we just don't know when more will be coming. So you may see more drug change requests from pharmacy. Also, since a lot of physicians are on this thread just a heads up as of 3-20-2020: 1 TITLE 22 EXAMINING BOARDS 2 PART 15 TEXAS STATE BOARD OF PHARMACY 3 CHAPTER 291 PHARMACIES 4 SUBCHAPTER A ALL CLASSES OF PHARMACIES 5 291.30. Medication Limitations. 6 No prescription or medication order for chloroquine, hydroxychloroquine, mefloquine, or 7 azithromycin may be dispensed or distributed unless all the following apply: 8 (1) the prescription or medication order bears a written diagnosis from the prescriber consistent 9 with the evidence for its use; 10 (2) the prescription or medication order is limited to no more than a fourteen (14) day supply, 11 unless the patient was previously established on the medication prior to the effective date of this 12 rule; and 13 (3) no refills may be permitted unless a new prescription or medication order is furnished. https://www.pharmacy.texas.gov/files_pdf/291.30.pdf If you get a call about these medications from pharmacy this is why. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Just heard from a buddy who is at Mt. Sinai in NY that they just adopted a mandatory DNR policy for COVID patients if via 2 physician consent it is determined a patient is unlikely to survive no matter what is done. I know first hand much of what the administration is stating in these pressers is false, because I see things to the contrary at my own facilities. I voted for Trump but it's extremely frustrating listening to him and those around him telling the American people things that just aren't true. Most major medical centers already have or are drafting plans with their legal departments for this scenario.*DNR* It's going to be implemented at more than a few before this is done. There are even medical and ICU directors at major institutions ON THE RECORD stating as much. Anything said to the contrary is, at best, misleading. Apparently the hospitals in NY are also starting run short on commonly used ICU meds, such as pressors and sedation. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ I am ER, trained at the Lake in BR We are doing plaq/azithro in the ICU....obviously we have the ability to keep them on the monitor if they go into Torsades. Agree, I am not testing anyone unless they are admitted. I am sorry, but I am not putting my nursing staff at risk for a mildly symptomatic patient to whom the treatment does not change, Intubation wise, trying to minimize risk as best as possible. I have the vent set up before hand, minimize bagging, have them on 100% NRB until RSI. Then I am pushing paralytic before hand to minimize sedation time. Tube them w glidescope and immediately put them on vent to decrease open circuit time. Can do this <90 sec if prepared. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
CRS, DrPH
Expert Level Adviser
Joined: January 20 2014 Location: Arizona Status: Offline Points: 26660 |
Post Options
Thanks(0)
Quote Reply
Posted: March 28 2020 at 1:59pm |
|
|
Here's the source: https://www.wxyz.com/news/coronavirus/henry-ford-hospital-leaked-memo-is-not-an-active-policy-but-plan-for-worst-case-scenario |
||
|
CRS, DrPH
|
||
|
||
|
Usk
V.I.P. Member
Joined: January 26 2020 Location: Virginia Status: Offline Points: 7325 |
Post Options
Thanks(0)
Quote Reply
Posted: March 28 2020 at 5:55pm |
|
|
|
||
|
||
|
Tabitha111
Adviser Group
Joined: January 11 2020 Location: Virginia Status: Offline Points: 11640 |
Post Options
Thanks(0)
Quote Reply
Posted: April 04 2020 at 12:34pm |
|
|
nurse in Rockland County, NY |
||
|
'A man who does not think and plan long ahead will find trouble right at his door.'
--Confucius |
||
|
||
|
Sheep Lady
V.I.P. Member
Joined: February 06 2020 Status: Offline Points: 3215 |
Post Options
Thanks(0)
Quote Reply
Posted: April 05 2020 at 6:56pm |
|
|
https://www.foxnews.com/us/detroit-er-nurse-dies-alone-at-home-from-coronavirus Unspeakable tragedy. She worked at Henry Ford Hospital. Prayers for family and friends. |
||
|
Sheep Lady
|
||
|
||
|
FluMom
Adviser Group
Valued Member Since 2006 Joined: February 03 2020 Location: Colorado Status: Offline Points: 14695 |
Post Options
Thanks(0)
Quote Reply
Posted: April 05 2020 at 8:06pm |
|
|
Think the heavy load of virus is why doc and nurses are dying. They breath a lot of the virus in and it is too much for their bodies. I think the load of virus is important...but I am no scientist! |
||
|
||
|
CharmlessMan
V.I.P. Member
Joined: February 09 2020 Status: Offline Points: 250 |
Post Options
Thanks(0)
Quote Reply
Posted: April 05 2020 at 11:46pm |
|
|
As Flumom just mentioned, Viral load does indeed appear to be a factor which is affecting the death rate amongst front line medical staff. There have been several articles published about this over the last couple of weeks: https://www.cebm.net/covid-19/sars-cov-2-viral-load-and-the-severity-of-covid-19/ Quote below is from the Guardian article: Edward Parker at the London School of Hygiene and Tropical Medicine said "For Covid-19, early reports from China suggest that the viral load is higher in patients with more severe disease, which is also the case for Sara and influenza." |
||
|
||
|
CRS, DrPH
Expert Level Adviser
Joined: January 20 2014 Location: Arizona Status: Offline Points: 26660 |
Post Options
Thanks(0)
Quote Reply
Posted: April 05 2020 at 11:50pm |
|
|
Yep, we call it "infectious dose." Putting patients on ventilators is about the riskiest part of the medical procedure = it generates all sorts of bodily fluids that can aerosolize and infect nurses, techs and doctors. It is cruel to expose our healthcare workers to these conditions....If I didn't have adequate PPE, I'd walk off of the job. |
||
|
CRS, DrPH
|
||
|
||
|
Technophobe
Assistant Admin
Joined: January 16 2014 Location: Scotland Status: Offline Points: 88450 |
Post Options
Thanks(0)
Quote Reply
Posted: April 06 2020 at 3:39am |
|
|
The wartime analogy works perfectly as an explanation for infectious dose. If a spearhead force of a few dozen squaddies goes 'over the top' they are easily shot down. But a huge invasion force like 'the D Day landings' is much harder to repel. (and yes, that includes using the eyes as a 'secret passage' that is unguarded) Exhaustion from overwork, dehydration from lack of breaks and vitamin D deficency from being under artificial light all shift - all contribute as well to weaken the 'home guard' of the immune system. |
||
|
How do you tell if a politician is lying?
His lips or pen are moving. |
||
|
||
|
Sheep Lady
V.I.P. Member
Joined: February 06 2020 Status: Offline Points: 3215 |
Post Options
Thanks(0)
Quote Reply
Posted: April 06 2020 at 6:32am |
|
|
So would I. They are using the best and brightest, many of those in their prime years of their career and they are using them like cannon fodder, not to mention many are seeing wage cuts. |
||
|
Sheep Lady
|
||
|
||
|
Post Reply
|
|
 Tweet
Tweet
|
| Forum Jump | Forum Permissions You cannot post new topics in this forum You cannot reply to topics in this forum You cannot delete your posts in this forum You cannot edit your posts in this forum You cannot create polls in this forum You can vote in polls in this forum |








 Topic Options
Topic Options MamaBear4 wrote:
MamaBear4 wrote: